

Prelude: This article is intended for healthy adults looking to maximize exercise-induced adaptations such as muscle hypertrophy and strength. This article is not intended to discuss the role of CBD Oil in individuals with anxiety disorders or medical issues.
I wrote this article due to a large amount of perfectly healthy individuals promoting CBD Oil and I will address the effects of CBD for a healthy population without anxiety disorders or medical conditions.
Table of Contents
What Is It? Will It Get Me High?
Cannabinoids are lipophilic ligands that bind to cannabinoid receptors (CB). There are three groups of cannabinoids that bind to cell-surface cannabinoid receptors;
1] Phytocannabinoids
2] Endocannabinoids
3] Synthetic cannabinoids.
Perhaps the most famous one is Δ9‐tetrahydrocannabinol (THC), this is the cannabinoid in marijuana that causes the “high” and euphoria as well as its analgesic, anti-inflammatory and psychoactive properties. Due to its psychoactive nature and legality in many places, usage of THC for these purposes is limited (Śledziński et al., 2018). Cannabidiol, or CBD Oil, is an extract from the hemp plant. CBD Oil has a very low concentration of the famous THC. Due to the low concentration of THC, CBD will not cause you to get high (Spielberger et al., 1983).
Receptors
Your body has many receptors which bind to their substrate to exert their action. Most receptors can bind to more than one substrate; their inclination to bind a specific substrate is called their affinity.
There are two primary cannabinoid receptors: CB1 and CB2. CB1 is mainly present in the central nervous system and brain, while CB2 is found in the peripheral nervous system and in immune cells.
Most of the effects of THC seems to be on CB1. The CB1 receptors have effects on short-term memory, motor function and movement, among others (Pertwee et al., 1997). Many of the psychoactive effects of THC seem to be due to its action on CB1 receptors; this makes sense, as the “high” from marijuana typically affects these functions. The CB2 receptors are located in the peripheral nervous system but have also been found on immune cells among a few other places. A good deal of the research on the effects of cannabinoids goes into understanding how CB2 can affect the immune system.
While there is positive research on modulation of the CB-receptors, it is important to note that CBD has a very low affinity for these receptors, meaning that when you consume CBD, it doesn’t actually bind to the CBD receptors in a major way. It is important to make this distinction because often, CBD companies will cite research about some exciting benefits found from CB-receptor action – but they don’t tell you that CBD has very low effect on these receptors. Although the mechanisms of CBD action are not fully understood yet, it seems to mainly interact with GPR55, TRPV1, TRPM8 receptors (Pertwee et al., 2010).
The Dosage and Proposed Benefits
As I discuss the effects of CBD observed in various studies, it is important for you to have context of what the marketed dosages are and what the proposed benefits are. A search of popular CBD companies revealed that most sell CBD in a dropper that contains contained 15-25mg of CBD per drop.
Further, most companies that sell CBD focus on the effects on sleep, anxiety, inflammation and recovery. I will go over these points and how they relate to healthy individuals looking to maximize exercise-induced adaptations.
Effects on Sleep
In a study by Nicholson et al. (2004), the effects of CBD and THC were tested on healthy adults. This study was a double-blind, placebo-controlled, 4-way crossover design; this means there were 4 different treatments and all subjects received all 4 treatments at different times, but neither the authors nor the subjects knew who was receiving which treatment when.
The four treatments were:
- 15mg THC
- 5 mg THC combined with 5 mg cannabidiol (CBD)
- 15 mg THC combined with 15 mg CBD
- Placebo.
The researchers measured next-day cognitive performance and memory, mood, fatigue, sleepiness and subjective ratings of sleep quality. Sleep latency was measured using an electroencephalogram; sleep latency is defined as the time that it takes you to actually fall asleep.
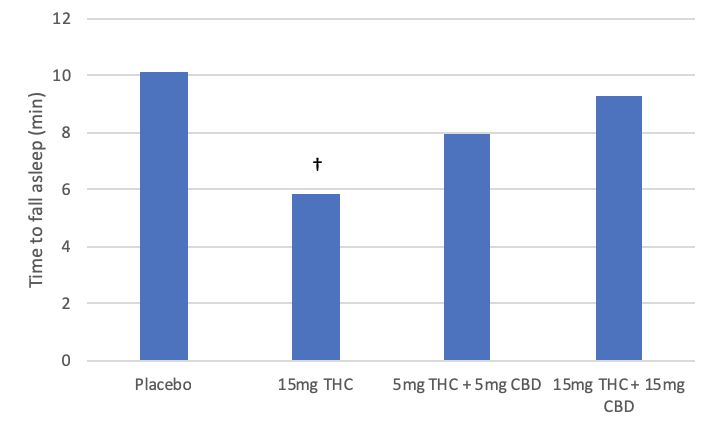
Figure 1. Sleep latency in placebo, THC, and THC + CBD. (Nicholson et al., 2004)
† Denotes statistical significance (p<0.05)
Compared to placebo, when subjects received 5mg THC + 5mg CBD or 15mg THC + 15mg CBD, there was a decrease in stage 3 sleep time and an increase in wakefulness. Further, the groups that received CBD oil took significantly longer to fall asleep than the ones that received THC alone. Additionally, the groups that received THC+CBD had no differences in time to fall asleep compared to placebo.
15mg of THC resulted in next-day memory impairment, however, resulted in a decrease in sleep latency. Thus, it seems that THC by itself can decrease the time to fall asleep while CBD increases that time, while also promoting wakefulness.
Effects on Anxiety
An important question to ask when looking at the effects that “X” may have on “Y” is: compared to what and in who? By that, I mean that we need to look at the population of people that the treatment is given to and what it is being compared to. I will focus on the studies performed on healthy subjects without anxiety disorders.
THC has been shown to have anxiogenic effects at high dosages; meaning it can make you anxious (Childs et al., 2017). Whether you have experienced it yourself, or have seen someone else experience it, you probably know of someone who smoked weed and thought that everyone knew and was out to get them. Those are the anxiogenic effects.
Many claim that CBD has anxiolytic (anxiety-suppressing) effects; now let’s ask ourselves: compared to what and in who?
In a study by Karniol et al. (1974), subjects received either:
- Placebo
- 15mg CBD
- 30mg CBD
- 60mg CBD
- 30mg THC
- 30mg THC + 15mg CBD
- 30mg THC + 30mg CBD
- 30mg THC + 60mg CBD.
The researchers measured pulse rate and subjective measurements of how the subjects were feeling and their sensations.
It was found that CBD alone did not have any effects on anxiety, while 30mg of THC increased it. It was also found that 30mg of THC significantly increased pulse rate. When THC and CBD were given in combination, it seems that CBD decreased the THC-induced anxiety effects. Thus, in this study we see that CBD can reduce anxiety in people who had THC-induced anxiety – this is different from saying that CBD can reduce anxiety in people with generalized anxiety, social anxiety, state anxiety or other types of anxiety.
A recent study by Linares et al., (2018) agrees with the results from Karniol et al (1974). In this study, 27 participants were randomized into a CBD group (300mg) or placebo. The researchers used a Visual Analogue Mood Scale, State-Trait Anxiety Inventory, Epworth Sleepiness Scale, Pittsburgh Sleep Quality Index, Adult Intelligence Scale and Psychomotor Vigilance Scale. Further, polysomnography parameters such as total sleep time (TST), sleep latency, rapid eye movement, sleep efficiency and many others were tracked. In short – this study tracked a lot of very relevant measures.
They received either 300mg of CBD or placebo 30min before the polysomnography tests started, which can be presumed to also be the time they went to bed.
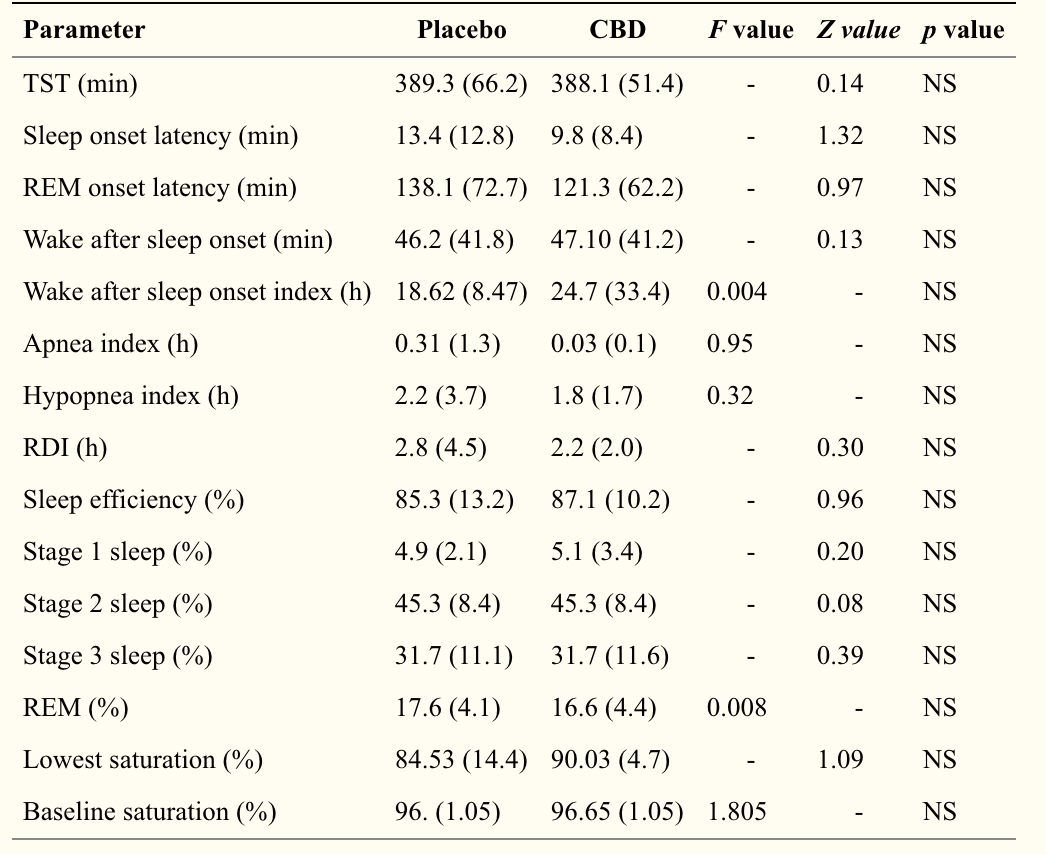 Figure 2. Measures of sleep taken by Linares et al. (2018).
Figure 2. Measures of sleep taken by Linares et al. (2018).
The researchers found no difference in any of the sleep or anxiety measures when comparing the CBD group to placebo. As you can see above, there is no statistical difference or even any consistent trends. Thus, here we see that in healthy adults with no-induced anxiety, CBD does not seem to have beneficial effects.
Another study looked at effects of 8mg THC, 16mg CBD and 8mgTHC + 16mgCBD or placebo in 48 volunteers that were either low or high-frequency cannabis users (Hindocha et al., 2015). Of interest to this article, this study measured trait anxiety using the Spielberger State-Trait Anxiety Inventory (Spielberger et al., 1983) before and after treatment. Further, they used a 10-point Visual Analogue Scale to measure how “stoned” the subjects were (this is actually the wording used). This was taken 15 minutes before treatment, 2 min after and then at 30, 60, 90 and 120 minutes after.
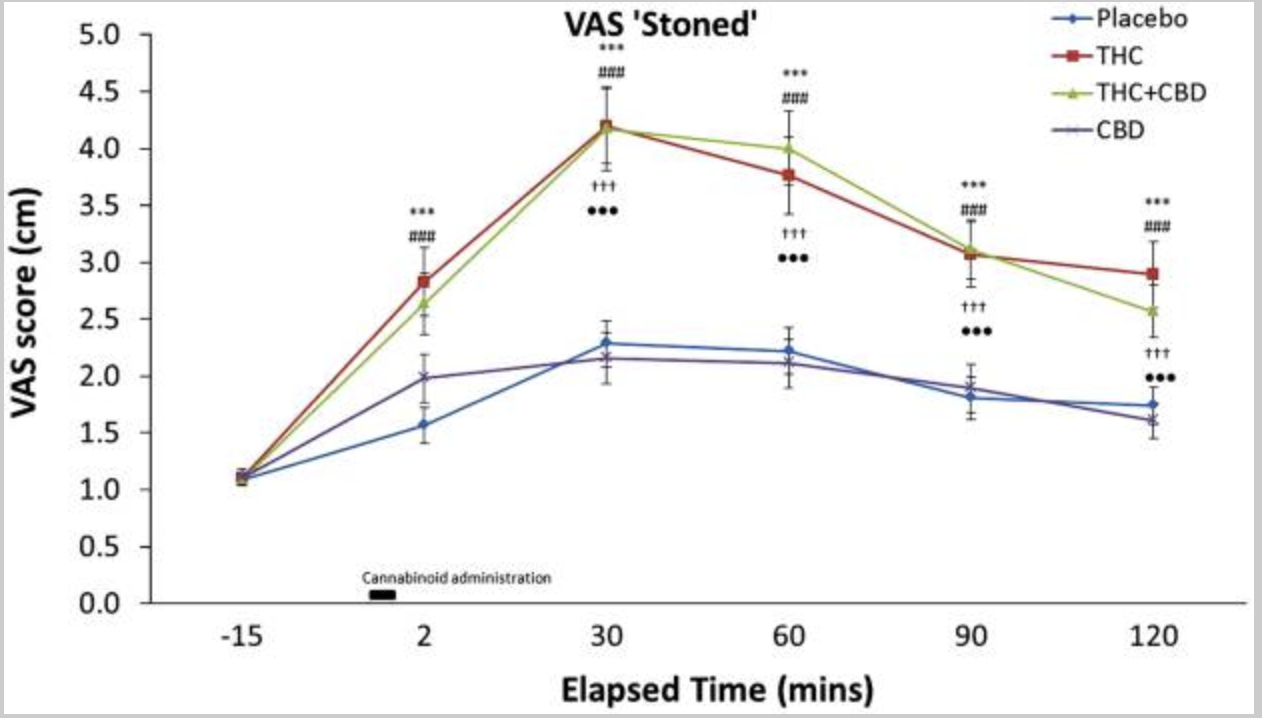 Figure 3. Visual analogue scale measurement of “stoned” level (Hindocha et al., 2015)
Figure 3. Visual analogue scale measurement of “stoned” level (Hindocha et al., 2015)
It was found that CBD alone did not cause subjects to feel stoned compared to placebo; while THC and THC+CBD both caused the same level of being stoned.
Further, it was found that CBD did not cause any differences in ratings of anxiety, alertness of happiness compared to placebo.
From the research above, it seems that CBD has no impacts on healthy adults without anxiety disorders. It is important to understand that there is a distinct difference between being acutely anxious over an exam, date or deadline and having a chronic anxiety disorder. Most of us get acutely anxious over certain events or concerns we might have, but that does not mean that you have an anxiety disorder. This article reviews the literature on healthy adults without anxiety disorders.
Inflammation and Immune System
There is an obsession with inflammation; yet, most people don’t understand what inflammation truly is and that it is necessary for muscle growth. Muscles fibres have command centres called myonuclei, one of their function seem to be to mediate work-induced hypertrophy. It seems that there is a threshold of muscle growth you can have before you need a greater number of myonuclei for further growth.
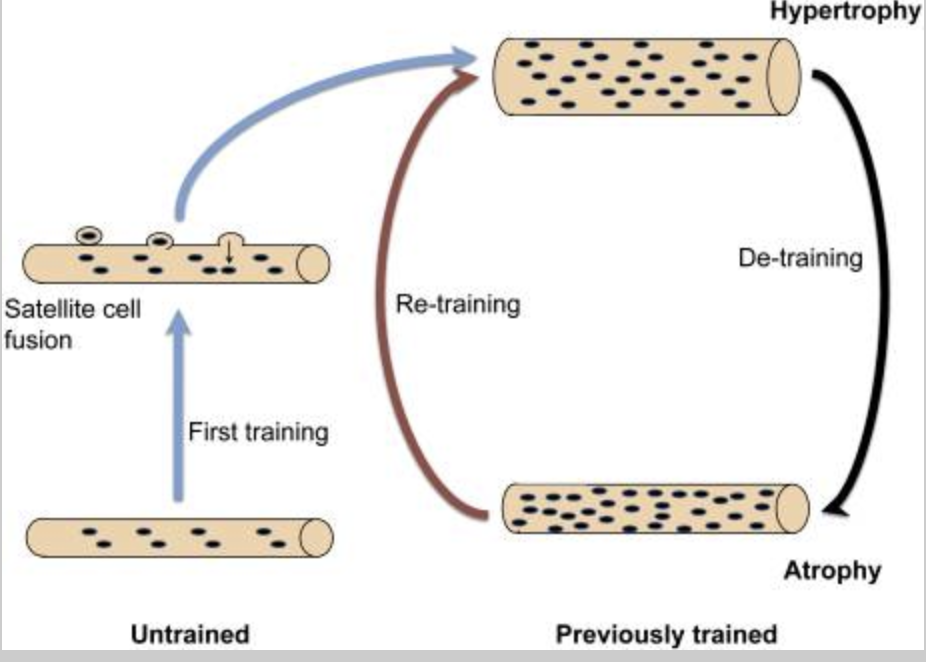
Figure 4. Satellite cell fusion to increase myonuclear domain, allowing further growth (Gunderson et al., 2016)
Enter satellite cells. In short, these cells donate myonuclei and allow further growth (although aspects of Myonuclear Domain Theory are being called into question). IL-6 is an intriguing cytokine, which can act as a pro-inflammatory and anti-inflammatory. It seems to have pro-inflammatory effects post-workout that have important roles in muscle hypertrophy. Specifically, it seems to regulate satellite cell proliferation for skeletal muscle hypertrophy (Serrano et al., 2008).
In a study by Mitchel et al. (2013), it was shown that elevated resting levels of IL-6 were inversely correlated to muscle growth while acutely elevated level of IL-6 post training was positively correlated to muscle growth. In other words; an acute inflammatory response post-workout seems to be beneficial for muscle growth. This study is a perfect example of why science cannot be taken as black-or-white, we need to consider all shades of grey and their context.
Interestingly, you can actually suppress muscle gain by constantly taking Non-Steroidal Anti-Inflammatory Drugs (NSAIDS) post-workout (Lilja et al., 2017). It seems that NSAIDs have an inhibitory effect on IL-6 as well as cyclooxygenase (COX) enzymes, which regulate two prostaglandin proteins called PGF2a and PGE2 that have roles on skeletal muscle protein synthesis. In fact, low levels of PGF2a have been correlated with lower protein synthesis and decreased Type I and II fibre size (Gibson et al., 1991).
A review by Merry & Ristow (2016), showed that antioxidant supplementation can also interfere with overload-induced muscle hypertrophy. Specifically, it seems that suppressing Reactive Oxygen Species (ROS) post-training may interfere with anabolic signalling.
The point of this is to tell you the following:
Do not fall trap to a product just because it claims to be able to reduce inflammation, have antioxidant benefits and be able to reduce ROS. The human body rarely works in absolutes.
Let’s get back to the topic of CBD though.
An in vitro study showed that CBD can inhibit the COX enzymes and production of prostaglandins (Ruhaak et al., 2011). As mentioned above, prostaglandin PGF2a and PGE2 have positive roles in muscle protein synthesis. Further, CBD does seems to reduce levels of IL-6 in humans (Vuolo et al., 2015). In contrast to NSAIDs and anti-oxidants, we simply do not have research on the effects of CBD on skeletal muscle hypertrophy. We can discuss mechanistic data until our faces turn blue, but the truth is that we need research looking at how CBD Oil consumption at various times in relation to a training session can affect acute and chronic muscle hypertrophy. I am not giving you this information so that you can turn around and say “See, I told you CBD is bad” or, “See, I told you CBD is good”. I am giving you information that will allow you to truly question whether CBD has a positive, negative or neutral impact on muscle hypertrophy and other exercise-induced adaptations.
Further, I am also not saying that we want inflammation and shouldn’t take a thing that suppresses it; low-grade chronic inflammation is related with a wide variety of nasty diseases, not to mention low testosterone levels and decreased muscle hypertrophy (Maggio et al., 2014; Norheim et al., 2017). Simply, I am saying that we do not have sufficient information yet to know whether CBD will have positive, neutral or beneficial roles in exercise adaptations such as hypertrophy and strength.
Recovery
Recovery from training is affected by several factors, including:
- Nutrition, sleep
- Total training volume
- Stress
- Menstrual cycle
- Number of stressful events
- Many others.
The three biggest influences on recovery are:
- Total training volume
- Nutrition
- Sleep
If you train at volumes that supersedes your ability to recover, you will find there is no amount of nutrition and sleep to allow for recovery. Similarly, a severe calorie deficit is going to severely restrict your ability to recover from training and will likely reduce the volume you can recover from. Inadequate sleep will interfere with your ability to tolerate high training volumes and maximally grow (Knowles et al,., 2018).
Typically, one can quantify recovery by testing peak strength, work capacity, maximum velocity contraction, subjective visual analogue scales of various ratings, various exercise measures such as the height or distance of a jump among many others. Since we do not have literature on the effects of CBD on these measures, we need to speculate about the effects that it could have on recovery. In my opinion, it is fair to assume that CBD Oil will not supercede the importance of training with adequate volume, nutrition or sleep. If recovery from training is your primary concern, then it will likely be much more beneficial for you to get your nutrition, training, sleep and relaxation on point before considering CBD Oil, or any “recovery” supplements for that matter.
Conclusion
We do not have enough evidence to support the usage of CBD Oil in healthy adults without anxiety disorders or not in a diseased state. Again, this article is not meant to discuss effects on people with disorders or diseases, as that is outside of our scope of practice. This articles reviewed the literature on healthy populations looking to maximize resistance training adaptations.
It seems that in healthy individuals, CBD does not improve quality of sleep, total sleeping time or shorten the time it takes to fall asleep compared to placebo (Linares et al, 2017; Nicholson et al., 2004). Further, compared to placebo it failed to reduce anxiety in people without anxiety disorders. CBD does seem to reduce anxiety in individuals with THC-induced anxiety or paranoia (Karniol et al., 1974).
The roles of CBD on the immune system and inflammation in non-diseased states still needs further research. Specifically, it is unknown if the anti-inflammatory and anti-oxidative effects of CBD could affect muscle hypertrophy, as taking NSAIDS or anti-oxidants post-training can interfere with growth (Gibson et al., 1991; Merry & Ristow, 2016). It would be interesting to see volume-equated research in a group of healthy, resistance-trained population taking CBD compared to placebo and observe effects on muscle hypertrophy, damage, recovery, strength and ratings of fatigue.
Until further research is conducted, I remain sceptical and doubtful about the effects of CBD in healthy adults looking to maximize exercise adaptations such as strength and hypertrophy.
Author
References
Bruusgaard, J. C., Johansen, I. B., Egner, I. M., Rana, Z. A., & Gundersen, K. (2010). Myonuclei acquired by overload exercise precede hypertrophy and are not lost on detraining. Proceedings of the National Academy of Sciences of the United States of America, 107(34), 15111-6.
Childs, E., Lutz, J., & De Wit, H. (2017). Dose-related effects of delta-9-thc on emotional responses to acute psychosocial stress. Drug and Alcohol Dependence, 177, 136-144. doi:10.1016/j.drugalcdep.2017.03.030
Gibson, J., Poyser, N., Morrison, W., Scrimgeour, C., & Rennie, M. (1991). Muscle protein synthesis in patients with rheumatoid arthritis: Effect of chronic corticosteroid therapy on prostaglandin f2 alpha availability. European Journal of Clinical Investigation, 21(4), 406-12.
Gundersen, K. (2016). Muscle memory and a new cellular model for muscle atrophy and hypertrophy. The Journal of Experimental Biology, 219, 235-42. doi:10.1242/jeb.124495
Hindocha, C., Lawn, W., Freeman, T., & Curran, H. (2017). Individual and combined effects of cannabis and tobacco on drug reward processing in non-dependent users. Psychopharmacology, 234(21), 3153-3163. doi:10.1007/s00213-017-4698-2
Karniol, I., Shirakawa, I., Kasinski, N., Pfeferman, A., & Carlini, E. (1974). Cannabidiol interferes with the effects of δ 9-tetrahydrocannabinol in man. European Journal of Pharmacology, 28(1), 172-177. doi:10.1016/0014-2999(74)90129-0
Knowles, O., Drinkwater, E., Urwin, C., Lamon, S., & Aisbett, B. (2018). Inadequate sleep and muscle strength: Implications for resistance training. Journal of Science and Medicine in Sport, 21(9), 959-968. doi:10.1016/j.jsams.2018.01.012
Linares, I., Guimaraes, F., Eckeli, A., Crippa, A., Zuardi, A., Souza, J., . . . Crippa, J. (2018). No acute effects of cannabidiol on the sleep-wake cycle of healthy subjects: A randomized, double-blind, placebo-controlled, crossover study. Frontiers in Pharmacology, 9, 315-315. doi:10.3389/fphar.2018.00315
Maggio, M., De Vita, F., Lauretani, F., Nouvenne, A., Meschi, T., Ticinesi, A., . . . Ceda, G. (2014). The interplay between magnesium and testosterone in modulating physical function in men. International Journal of Endocrinology, 2014, 1-9. doi:10.1155/2014/525249
Merry, T., & Ristow, M. (2016). Do antioxidant supplements interfere with skeletal muscle adaptation to exercise training? The Journal of Physiology, 594(18), 5135-47. doi:10.1113/JP270654
Mitchell, C., Churchward-Venne, T., Bellamy, L., Parise, G., Baker, S., & Phillips, S. (2013). Muscular and systemic correlates of resistance training-induced muscle hypertrophy. Plos One, 8(10), 78636. doi:10.1371/journal.pone.0078636
Nicholson, A., Turner, C., Stone, B., & Robson, P. (2004). Effect of delta-9-tetrahydrocannabinol and cannabidiol on nocturnal sleep and early-morning behavior in young adults. Journal of Clinical Psychopharmacology, 24(3), 305-13.
Norheim, K., Cullum, C., Andersen, J., Kjaer, M., & Karlsen, A. (2017). Inflammation relates to resistance training-induced hypertrophy in elderly patients. Medicine and Science in Sports and Exercise, 49(6), 1079-1085. doi:10.1249/MSS.0000000000001221
Śledziński, P., Zeyland, J., Słomski, R., & Nowak, A. (2018). The current state and future perspectives of cannabinoids in cancer biology. Cancer Medicine, 7(3), 765-775. doi:10.1002/cam4.1312
Spielberger C.D., Gorsuch R.L., Lushene R., Vagg P.R., Jacobs G.A. Consulting Psychologists Press; Palo Alto, CA: 1983. Manual for the State-Trait Anxiety Inventory (Form Y)
Pertwee, R. (1997). Pharmacology of cannabinoid cb1 and cb2 receptors. Pharmacology & Therapeutics, 74(2), 129-80.
Pertwee, R., Howlett, A., Abood, M., Alexander, S., Di, M., Elphick, M., . . . Ross, R. (2010). International union of basic and clinical pharmacology. lxxix. cannabinoid receptors and their ligands: Beyond cb₁ and cb₂. Pharmacological Reviews, 62(4), 588-631. doi:10.1124/pr.110.003004
Ruhaak, L., Felth, J., Karlsson, P., Rafter, J., Verpoorte, R., & Bohlin, L. (2011). Evaluation of the cyclooxygenase inhibiting effects of six major cannabinoids isolated from cannabis sativa. Biological & Pharmaceutical Bulletin, 34(5), 774-8.
Vuolo, F., Petronilho, F., Sonai, B., Ritter, C., Hallak, J., Zuardi, A., . . . Dal-Pizzol, F. (2015). Evaluation of serum cytokines levels and the role of cannabidiol treatment in animal model of asthma. Mediators of Inflammation, 2015, 538670-538670. doi:10.1155/2015/538670
What Next?
Join our free facebook group or add us on Instagram (revivestronger) and ask your question there, I will respond asap. Or if you’re after a fresh training programme we have a free 4 week plan using DUP that you can download for free here.
One more thing…
Do you have a friend who would love the above?
Share this article with them and let me know what they think.
[bctt tweet=”CBD Oil worth the hype? Anxiety, Sleep, Inflammation and Muscle” username=”revivestronger”]